

It started as a search for cutting-edge SCI rehab possibilities, but before long a newly-injured 17-year-old gymnast and her family had traveled thousands of miles and visited dozens of rehab and research centers. Then came the six-figure financial commitment, years of dedicated daily exercise, and finally, a hint of motor function returning. It was a beginning, and no one knew where it would lead.

I met Jessica Harthcock, now 27, last March when I was covering a trade show for NEW MOBILITY. She is the founder of the Tennessee chapter of the National Spinal Cord Injury Association — the membership arm of United Spinal Association. I struck up a conversation with her at the NSCIA booth about her beautiful service dog Ozzie, an English lab that stayed glued to her side as she walked about. I asked if she was a service dog trainer. “No, I’m a paraplegic and Ozzie’s my service dog,” she replied.
A walking paraplegic? After I remarked that her injury must be very incomplete and jokingly offered to trade injuries with her, she explained her original diagnosis was T3 complete and she didn’t get any return for almost two years, and that right out of rehab she embarked on a path of daily, often cutting-edge therapy, to get to this point.
My immediate thoughts were: Therapy that creates functional return in a complete SCI? No way! Not possible! But as a journalist I tried to stay open-minded and asked to hear her story. Fascinating as it is, I’m still trying to wrap my mind around it.
The Quest for Return of Function
Harthcock was a competitive springboard diver, dancer and gymnast when on June 7, 2004, at age 17, she crashed while doing a gymnastics maneuver. At the instant of injury the immediate effects were momentary paralysis from the neck down and a serious head gash, but in a few minutes she was able to walk away from the accident with the help of two people. She was driven to a hospital ER, evaluated, stitched up and sent home.

Five days later she returned to the hospital because her sensory and motor function had seriously deteriorated — to the point of near complete paralysis. Tests showed fractured vertebrae from C6 to T5 and a cyst encircling T3-4. Three days later, at a different hospital, she had an operation to remove the cyst, and the fractures were stabilized with plates. At this time tests indicated that she had complete paralysis at the T3-4 level.
“After surgery I woke up and thought, ‘what the heck, how come I still can’t feel or move my legs?’” she recalls. A nurse explained that the injury was permanent and she would go through rehab and learn how to use a wheelchair. Thus began a chapter in Harthcock’s life of relentlessly searching for answers in the rehab world and total dedication to the task at hand — pursuing the goal of walking again.
She was transferred to Frazier Rehab Institute in Louisville, Ky., where she did five weeks of inpatient therapy, then returned home with her family in Evansville, Ind. Once home, she continued traditional physical and occupational therapy at a local rehab clinic three days a week for the next nine months — covered under the family’s stellar insurance policy through United Healthcare. With a competitive spirit and strong athletic drive, she did her daily therapy at home, stretching, building her upper body and mentally trying to move her legs.
“My family and I understood the severity of my SCI, but we weren’t going to accept the answer,” says Harthcock. “We wanted something to try, whether it was a treatment or a new therapy. We felt like we hadn’t exhausted all options.”

Shortly after coming home from Frazier, the family saw a television show about three people with complete SCI who participated in Lokomat (locomotor training) therapy, which utilizes a robotic device similar to an exoskeleton that suspends the participant on a treadmill where walking patterns are replicated. All three participants were now up and taking steps on their own with forearm crutches or walkers — each had gotten some return. Harthcock says she understands there were others who tried the therapy and didn’t get any return, but the success stories of these three participants spurred her and her family to look into locomotor training and any other therapy that might help her.
In the fall of ’04 Harthcock went back to finish her senior year of high school, attending classes in the morning, doing rehab afternoons. On school breaks she and her parents loaded into the family van and crisscrossed the country, visiting rehab centers and looking at therapy options. “We visited at least 25 rehab centers,” she says. In addition to traveling together as a family, her mother, Krista Greenfield, became Harthcock’s insurance advocate and did a lot of research into rehab options.
In April of 2005 Harthcock got a second opinion from Shriners Children’s Hospital in Chicago, essentially the same as the first. In early June, on the one-year anniversary of her injury, a doctor at the Mayo Clinic in Rochester, Minn., told her, “It has been a year since your injury and I think perhaps it’s time for you to accept your lot in life and move on. Go to college and you will do great.”
Still not satisfied, Harthcock and her family visited the University of Miami Hospital, where doctors Barth Green and Martina Arizolas told the family that some people recover and walk and some don’t, and the Miami Project is doing a lot of studies to figure out why.
Undaunted, she returned to Shriners Hospital for a 25-day inpatient stay of intense physical therapy along with strength and balance training. Shriners provides services free of charge to children under 21.
Two Years of Hard Work
In July 2005 she hired an athletic and personal trainer, Adam Harthcock, to help her continue to build on the strength and balance she had achieved at Shriners. They did three-hour sessions, two or three days a week. Hiring Adam was doubly rewarding — the two became close. After several months they began dating.

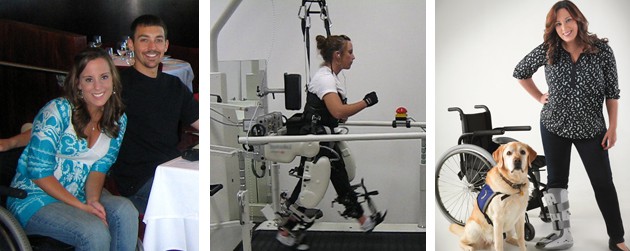
In January 2006 the family drove to Frazier Rehab again where she participated in an outpatient locomotor treadmill gait training study done by Dr. Susan Harkema, director of the Reeve Foundation’s NeuroRecovery Network. Since it was a study, there was no charge. At Frazier she went to therapy four to five days a week, five to six hours a day, including 90 minutes on the treadmill, plus strength, stretching and movement therapy. The family was living out of a hotel room.
In the evenings Harthcock took online classes for her undergraduate degree in public relations and mass communications at the University of Southern Indiana. Although her functional neurological status remained T3 complete, her strength and balance continued improving and, being double jointed, she learned how to “stand” without support by locking her knees. However, two months into the study, it was decided that Harthcock wasn’t making enough progress, and Harkema wanted to reduce her therapy to one or two days a week. For Harthcock this wasn’t enough. “At the time nothing was going to stop me,” she says. “I tend to be really stubborn, so when I get something in my mind, I typically get narrowly focused on it.”
Her focus led to NextSteps Chicago Spinal Cord Injury Center — also part of the NeuroRecovery Network. In late March 2006, her dad drove her to Chicago and moved her into a hotel near NextSteps and bid farewell. “Back then NextSteps was a small, private pay facility that had exactly the right ‘out of the box’ training and equipment, including a Lokomat,” she recalls.

At NextSteps, she would arrive early and stay late, extending two-hour sessions out to five and six hours, for five and sometimes six days a week — doing physical therapy, riding an ERGYS (FES) bike. And she finally got to use a Lokomat. “It felt great to be upright on the Lokomat — except the first time, when I passed out because I wasn’t used to being upright.”
Obsessively driven, she was spending her days at NextSteps and evenings doing online classes in her hotel room. Occasionally Adam would visit to spend time with her, and to learn the therapy techniques so he could work with her at a later date. “NextSteps was like going to boot camp, and I was putting 100 percent into my rehab and was loving it,” she says. “I really didn’t have a specific goal or timeframe. I always said, ‘I will do this for as long as it takes.’”
Her balance was much improved and she was in excellent shape — even the most difficult transfers had become a breeze — but she still had no neurological return. Then, 22 months post-injury, she noticed a muscle twitch in her right thigh. “At first I thought it was a muscle spasm, but I found I could make it ‘twitch’ or spasm when I intended.”
Taking It to the Max
Now, working her right thigh muscle was added to her training regime. Trainers would attach a bungee cord from her waist to her shoe, which put her leg in a bent position, and have her try and straighten the leg. They set her up with a portable electrical stimulator unit, which causes the muscle to flex. She would use it on and off for 20 minutes at a time several times a day.
After her stint at NextSteps, she went back to Shriners for another three-week intense session of inpatient therapy. Shriners orthotists made custom long leg braces and fit her with forearm crutches. She returned to NextSteps for another two months of therapy and to work with the leg braces, which started creating hip flexor movement.
That fall Harthcock attended USI on campus full-time, and with a personal trainer she continued with the rehab techniques she learned at NextSteps. “I pretty much led the sessions, telling the trainer what to do.”

By January 2007 Harthcock was experiencing so much voluntary muscle return — hip flexors and some quadriceps in both legs — that she wanted to ramp up her therapy even more. She switched back to online classes at USI and her mom managed to get her insurance to pay for two more months of inpatient therapy at Frazier. The amount of return she had gotten was so rare that doctors agreed to readmit her — which is also very uncommon — to help her maximize the return.
At Frazier her rehab therapy included underwater treadmill pools. With a treadmill on the floor of the pool, water is added to the pool to simulate whatever weight is needed for therapy. To use a treadmill pool, there must be enough voluntary muscle control to do some type of ambulation. Although Harthcock had some leg movement, she had no sensation.
A TV screen was set up in front of the pool so she could see what her legs were doing — a form of biofeedback. “I had the pool filled up to my neck. Working in the treadmill pool enabled me to control and improve my hip flexors.” In this two-month stint at Frazier she got strong enough to take steps using long leg braces and crutches. She still didn’t have any stomach muscle control, so balance was very difficult, but her years of tap, jazz and ballet dancing paid off in helping her compensate.
Right out of Frazier, she went back for yet another three weeks of inpatient therapy at Shriners, where she continued working in their therapy pool.

Photo by Rutherford Studios
By this time she and Adam were deeply in love. That fall she followed him to LSU. Adam worked as a strength coach for the LSU football team, which had world-class training facilities and underwater treadmill pools for player rehab. “They were very kind and let me use the workout facilities and underwater treadmills,” says Harthcock. “I kept working and working, setting tiny goals, making tiny gains every day.” She was still using a chair to get around campus and crutches and long leg braces to get around the house. She also threw herself into college life, joined a sorority and finished off her undergraduate degree in three years.
In the summer of 2008 Harthcock tried hippotherapy — therapeutic horseback riding. She did this two days a week, which greatly helped with trunk balance and core strengthening.
She continued to work on tiny goals and make tiny gains each day. By mid-2009 she was able to walk on her own without crutches or braces — the muscles in her lower legs that prevent foot-drop were the last to return — all the while having a full academic and social life.
Adam proposed in September 2009 and they were married in 2010. Jessica earned a masters degree from Vanderbilt in organizational leadership and Adam earned an MBA.
Today: A Walking Para
These days Harthcock walks nearly full-time, using a wheelchair only for long distances — zipping through the airport or around a mall, or if she is tired or sick. Her walking gait looks normal — a testament to her superior athleticism and balance learned from years of dance and gymnastics, as well as all the hard work. However, because she has no sensation or proprioception, she needs to be able to see to remain standing. She can’t stand in the dark, has to see every step she takes, and can’t tell that she has taken a step unless she sees it. She can’t voluntarily contract her abdominal muscles, but can activate them by leaning to one side or the other, for balance (the opposite side contracts).
She can’t feel if she has injured her legs. She has had broken toes and not known it, and during therapy she tore a ligament in her right ankle so badly that she had to wear a walking boot for two years. Today she is in a walking boot again for a ligament tear in the same ankle, incurred last July.
If she gets nudged, she will fall down. “I have to laugh about it, because I can’t get up from the ground. I have to say to nearby people, ‘I really can’t get up without your help.’” She also can’t bend over at the waist or knees, which is where Ozzie is a great help in picking things up for her.
Stairs are doable but difficult — she needs a handrail. Grass and uneven surfaces are very difficult, and she needs one or two people to hold onto if she is in sand. Curbs are also difficult, so she prefers curb cuts.
 Like other high-thoracic paras, she has no abdominal sensation, has no bowel and bladder control, and still struggles with autonomic dysreflexia, which she says seems to come back a lot. She says trying to explain which muscles she can use is complicated. For instance, she can advance her leg when she is standing, but has a hard time raising it when she is lying down. Her hip flexors are her strongest muscles, she says, and she also has control of her quadriceps.
Like other high-thoracic paras, she has no abdominal sensation, has no bowel and bladder control, and still struggles with autonomic dysreflexia, which she says seems to come back a lot. She says trying to explain which muscles she can use is complicated. For instance, she can advance her leg when she is standing, but has a hard time raising it when she is lying down. Her hip flexors are her strongest muscles, she says, and she also has control of her quadriceps.
Being able to walk and see people eye-to-eye is a big deal. It also has health benefits — she won’t have to worry about pressure sores, although she has to be careful to check where she is sitting so she doesn’t accidentally sit on a pair of glasses or car keys. She is also less likely to develop osteoporosis.
Adam and Jessica have taken the information and resources they have learned on this journey and are starting their own company, Utilize Health. Their business helps match people with neurological disabilities to their options so they can reach their maximum health and recovery by using information provided on therapy centers, options and resources.
Everybody has different commitments and resources, she says. “I suggest looking at additional rehab like going to the gym.” She understands there is no way to know what kind of recovery a person will get or how long it will take, but most of the people she knows who have gone to additional therapy have gotten something back. Sometimes it is being able to sit upright, while other times it may be gaining the function to walk with leg braces.
Looking back at the beginning of her quest, she says, “At that point in my life I was young and had no commitment, so I could take four years and devote to it. I was fortunate to have a supportive family and boyfriend. I was able to do school and put 100 percent into rehab, and I loved what I was doing.”
Now, married with a job, she knows it would be a lot more difficult. “But I would probably still try for a recovery — because that is my personality.”
Resources
• Reeve Foundation NeuroRecovery Network: christopherreeve.org
• Miami Project: miamiproject.miami.edu
• NextSteps Chicago: nextstepschicago.org
• Shriners Hospitals for Children: shrinershospitalsforchildren.org
• Utilize Health: utilizehealth.co
What is a ‘Complete’ SCI?
It’s essential to understand, says Reggie Edgerton, Ph.D. — whose clinical work has demonstrated that the spinal cord has memory and intelligence — that when we say “complete” SCI, the term is limited to what a person can or can’t feel or move. It is a physical exam that assesses current functionality. However, studies of countless MRIs show that a very high proportion of people with SCI who test as complete still have some intact nerve pathways, but those pathways are non-functioning. In other words, functional and anatomical assessments give us two very different views of paralysis.
The epidural stimulation trials at Frazier Rehab in Louisville have opened up an entirely new way of looking at complete and incomplete spinal cord injuries. Now the focus is on learning and understanding more about the specific pathways within the cord. Mapping the circuitry of the spinal cord may enable researchers to move beyond the often misleading terms of complete and incomplete and concentrate on specific — and more hopeful — potential outcomes.
What Enabled Harthcock’s Recovery?
Harthcock’s story is very unusual in terms of her determination and her financial resources, says Reggie Edgerton, the SCI researcher from UCLA who designed the Louisville epidural stimulation trial reported on in the September 2011 issue of NEW MOBILITY (“Rob Summers: From Quad to Para and Beyond?”.
Our experiments, he says, “show that we have underestimated the degree with which the brain and spinal cord can reorganize and recover function when there is activity-based therapy.” The most logical explanation for the return noted in the epidural stimulation trial in Louisville is there are still intact connections in the spinal cord, but they are so damaged that they can’t conduct an impulse. The locomotor training helps reroute signals to working connections, and the epidural stimulator then acts as a kind of hearing aid that amplifies the signal and enables some degree of muscle control below the level of injury.

Additional evidence for activity-based therapy can be found in Edgerton’s animal studies in which two groups of rats had transected spinal cords and were fitted with epidural stimulators. The first group was put on treadmill training for two weeks and the second wasn’t. The treadmill-trained rats gained recovery, while the second group had no recovery. Edgerton says this suggests that activity-based therapy is important in all types of recovery, including regeneration. “We know that the spinal cord learns, and it also forgets. It could be that you figure out a successful stem cell therapy that makes new connections, but the spinal cord circuitry is so untrained that it can’t respond.”
This doesn’t mean everybody will get return, or in the same timeframe and manner. There are no absolutes, says Andrea L. Behrman, co-director of the Reeve Foundation NeuroRecovery Network, and executive director of Kosair Charities Center for Pediatric NeuroRecovery in Louisville. “However, if I was injured, I would do some type of activity-based therapy.”
The way activity-based rehab empowers recovery, says Behrman, is based on plasticity — the brain’s ability to create new connections. Studies show the spinal cord has plasticity as well. In most cases of SCI there are still some intact neural pathways, but no information is getting through. When you attempt some type of movement, the brain sends signals down the spinal cord but signals can’t make it through the damaged, jumbled neural pathways at the injury site. Activity-based rehab below the lesion — like locomotor training or FES —causes the spinal cord to learn patterns, similar to patterns when learning to play a musical instrument. With repetition and specific sensory input, patterns become more ingrained and create a signal of excitability that tries to find an upward path to the brain. The more repetition, the stronger the signal. Perhaps if the old neural pathway is too damaged, the signal starts trying other neural pathways until it finds one that is intact enough to make it through and up to the brain.
Studies also support the theory that it is never too late for activity-based therapy to activate areas below the injury — even many years post injury, says Behrman. But like starting to learn a musical instrument, then stopping, then restarting again, the more years that go by, the longer it will take and the less activation you are likely to recover.
This new information opens up a world of possibilities and shows we have just scratched the surface of research that needs to be done. What are the optimum activity-based therapies, who can and cannot benefit, and how long will it take? Right now there is no way to know. One person may work for years and get recovery like Harthcock, while others may work just as long and the payoff may be activation of muscles that enable better transfers, or activation of more trunk muscles so that they can sit up better. Or in some cases, nothing.
“The goal from a scientific standpoint is to get to a point where we can tell a newly injured person, ‘With this injury, you have this likelihood of this much recovery. But to try and achieve that you will have to do this,’” says Edgerton. “If you tell somebody they will have to work their butt off for eight years, and the likelihood of what they may get back — then they know what the physical and financial costs will be, and they can make an educated decision whether to put in the money, time and effort. Or they can leave things as they are and get on with their lives. But we are a long way from this. That is why this research is so important,” he says.
Expenses of Therapy
When it comes to adding up the expenses in her quest for recovery, Harthcock’s figures show how fortunate she was in terms of insurance, but they also show her dedication not to take anything for granted and get the most out of every opportunity.
As for financial resources, her father, Dennis Greenfield, is in commercial real estate. Her mother, Krista, is a personal secretary and professional proofreader who became her full-time insurance advocate. Friends and family from her church and school did several large fundraisers that raised a total of $60,000 to help offset expenses.
Expenses included:
• Hotel costs and gas for the family’s full-size van while driving to visit 25 rehab facilities in 24 weeks. Airline tickets to the Miami Project, which was farther away.
• Approximately 48 weeks of a personal trainer, two or three times a week, 1.5 hours a day at $50 per hour. The trainer would usually work with her for three hours but only charge for 1.5 hours.
• Four months at NextSteps Chicago, $150 per two-hour session, plus $35 if Lokomat was included. Total for NextSteps stay, approximately $11,400.
• Nine months of three-day a week outpatient physical and occupational therapy at a rehab center near her home, covered under her insurance.
• Nine-weeks of inpatient rehab at Shriners Chicago, at no charge. Shriners estimates its cost is more than $3,000 per day. Plus Shriners provided custom long leg braces and forearm crutches at no charge.
• 17 extra weeks at Frazier rehab (nine as an outpatient — no charge because she was part of a study; eight weeks as an impatient covered under her insurance.
• Eight weeks of Hippotherapy 1-2 days a week.
• Three years free use of the LSU weight room and physical therapy center, including treadmill pool and biofeedback machine.
Support New MobilityWait! Before you wander off to other parts of the internet, please consider supporting New Mobility. For more than three decades, New Mobility has published groundbreaking content for active wheelchair users. We share practical advice from wheelchair users across the country, review life-changing technology and demand equity in healthcare, travel and all facets of life. But none of this is cheap, easy or profitable. Your support helps us give wheelchair users the resources to build a fulfilling life. |

Love your site!! Fantastic articles and keeps me current. Thanks. Peg